A forgotten number that somehow impacts the heart.
Many people have a long-standing habit of snoring, frequently waking up feeling tired, experiencing morning headaches or daytime sleepiness, along with other cardiovascular symptoms. When they seek medical care, they are diagnosed with hypertension, arrhythmias, or even coronary artery disease, but no clear cause is found.
In many cases, the real cause lies in sleep. Specifically, sleep apnea (OSA) – a common but often overlooked disorder.
The AHI index, measured during polysomnography, is the key to early detection of this condition. Beyond diagnosis, AHI is also crucial for assessing cardiovascular risk.
What is AHI? Understanding the AHI Index Correctly
AHI (Apnea-Hypopnea Index) is an indicator that shows the number of complete pauses in breathing or reduced breathing during each hour of sleep. It is the primary index used to diagnose sleep apnea.
An apnea event occurs when airflow is completely blocked for at least 10 seconds. In contrast, hypopnea refers to a significant reduction in airflow accompanied by a drop in blood oxygen levels or brief awakenings (arousals).
During polysomnography, the system records parameters such as airflow, oxygen concentration, heart rate, and electroencephalographic and electromyographic activity. Based on this data, the doctor calculates the total number of apnea and hypopnea events, then divides it by the total sleep time to arrive at the AHI index.
Regarding the classification of levels:
- AHI < 5: Normal
- AHI 5–15: Mild
- AHI 15–30: Average
- AHI ≥ 30: Severe

For example, if a person has an AHI of 30, it means that for every hour of sleep they experience approximately 30 respiratory interruptions. This situation, repeated continuously throughout the night, creates a significant physiological burden on the body.
Why does high AHI affect cardiovascular health?
The link between AHI and cardiovascular health is not coincidental. It stems from the repetitive physiological changes that occur during sleep.
Intermittent hypoxia
During sleep apnea, the oxygen level in the blood drops and then rises repeatedly. This phenomenon is called intermittent hypoxia.
This condition damages the endothelium of blood vessels, increasing the risk of atherosclerosis and promoting cardiovascular disease.
Increased sympathetic nervous system activity
Each time breathing stops, the body reacts as if it were in a state of stress. The sympathetic nervous system is activated, increasing heart rate and blood pressure.
If this happens hundreds of times every night, it will lead to chronic hypertension, especially high blood pressure at night.
Oxidative stress and inflammation
Repeated oxygen deprivation increases the production of free radicals and inflammatory mediators. This is a fundamental mechanism in the formation and progression of coronary artery disease and stroke.
Changes in chest pressure
While struggling to breathe when the airway is obstructed, the negative pressure in the chest cavity increases significantly. This increases the burden on the heart, which over time can lead to ventricular hypertrophy and heart failure.
The link between AHI and serious cardiovascular diseases
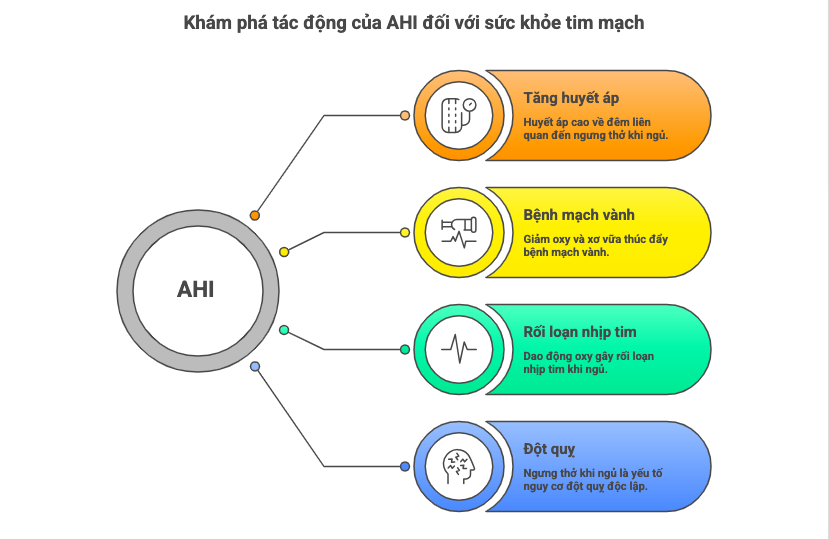
High blood pressure, especially high blood pressure at night.
In healthy individuals, blood pressure tends to decrease during sleep. However, this does not happen in people with sleep apnea. Blood pressure may not decrease or may even increase during the night.
This type of blood pressure is called “non-dipping” and is strongly associated with an increased risk of stroke and target organ damage.
Coronary artery disease
Sleep apnea reduces oxygen supply to the heart muscle and promotes atherosclerosis. People with high AHI, especially severe levels, have a significantly higher risk of coronary artery disease compared to the general population.
Heart rhythm disorders
Constant fluctuations in oxygen and nervous activity can cause arrhythmias such as atrial fibrillation, premature beats, or bradycardia during sleep.
Stroke
Numerous studies have identified sleep apnea as an independent risk factor for stroke. This risk increases with the level of AHI.
What AHI levels are dangerous for cardiovascular health?
Cardiovascular risk does not appear suddenly but increases gradually with the level of AHI.
- From AHI 5–15: early effects on blood pressure begin to appear.
- From AHI 15–30: cardiovascular risk increases significantly.
- AHI ≥ 30: high risk for stroke, coronary artery disease, and arrhythmias.
However, the AHI index does not reflect the entire level of danger. Two people with the same AHI but different levels of oxygen deprivation may have very different cardiovascular risks.
Hypoxic burden – an additional factor for more accurate AHI assessment.
In recent years, studies have shown that hypoxic burden can predict cardiovascular risk better than AHI.

This concept not only counts the number of breath-holding episodes but also takes into account:
- How severe is the oxygen reduction?
- How long does it last?
- Total time the body is in a state of oxygen deprivation.
A study published in the journal Chest showed that hypoxic burden is strongly associated with cardiovascular mortality risk, while AHI alone is not always an accurate predictor.
This has significant implications in clinical practice. A patient with moderate AHI but deep and prolonged hypoxemia may still face a high cardiovascular risk.
When is polysomnography needed to check for AHI?

You should consider polysomnography if you experience the following symptoms:
- Loud, prolonged snoring, sometimes with periods of apnea.
- Daytime sleepiness or decreased concentration
- Difficult-to-control hypertension
- Cardiovascular disease of unknown cause
- Overweight or obese
Currently, in addition to measurements taken at hospitals, many facilities have implemented home polysomnography, making screening more accessible for patients.
Does lowering AHI help protect cardiovascular health?
Treatment of sleep apnea, particularly with CPAP, has been shown to offer numerous cardiovascular benefits.
CPAP helps maintain an open airway throughout sleep, thereby reducing the number of apnea episodes and improving blood oxygenation.
Studies show that regular CPAP use may:
- Lowering blood pressure, especially nighttime blood pressure.
- Improve heart function
- Reduce the risk of stroke.
Treatment effectiveness depends decisively on patient compliance. Medical standards recommend that patients use a CPAP machine for at least 4 hours each night and maintain this consistently for over 70% of the total number of nights.
Conclude
The AHI index is an important tool in diagnosing and assessing the severity of sleep apnea. However, to fully understand cardiovascular risk, additional factors such as hypoxic burden need to be considered.
Early detection and timely treatment not only improve sleep quality but also play a crucial role in preventing serious cardiovascular events.
If you have any suspicious symptoms, undergoing polysomnography is a necessary step to protect your long-term health.
Frequently Asked Questions
At what AHI level does treatment become necessary?
Generally, an AHI of 15 or higher requires evaluation and consideration of treatment, especially when accompanied by symptoms or underlying medical conditions.
Does sleep apnea cause high blood pressure?
Yes. This is one of the common causes of difficult-to-control high blood pressure.
Are home polysomnography (sleep tracking) methods accurate?
In many cases, this method is accurate enough for initial screening and diagnosis.
References
- Azarbarzin A et al. The hypoxic burden of sleep apnea predicts cardiovascular disease-related mortality. American Journal of Respiratory and Critical Care Medicine.
https://www.atsjournals.org/doi/full/10.1164/rccm.201807-1326OC - Oldenburg O et al. Sleep-disordered breathing in patients with heart disease. European Heart Journal.
https://academic.oup.com/eurheartj/article/37/27/1953/1748917 - Javaheri S, Barbe F, Campos-Rodriguez F et al. Sleep apnea and cardiovascular disease. American Heart Association.
https://www.ahajournals.org/doi/10.1161/CIR.0000000000000988 - Azarbarzin A et al. Association of hypoxic burden with cardiovascular mortality. Chest Journal.
https://journal.chestnet.org/article/S0012-3692(19)34412-2/fulltext - Malhotra A et al. Metrics of sleep apnea severity: beyond the apnea-hypopnea index. Sleep.
https://academic.oup.com/sleep/article/43/10/zsaa148/5864007
SleepFi Clinic
Address: 114 Street No. 32, Sub-district 1, An Lac Ward, Ho Chi Minh City
Hotline: 0916872112

